To lose 10 pounds in a month is one of the most common fitness goals, but if you search the internet, you’ll find a lot of dangerous advice. Extreme crash diets and exhausting 3-hour workouts might give you quick results, but they usually lead to burnout, muscle loss, and gaining the weight right back.
At me-fitter.com, we believe in getting fitter the right way.
Losing 10 pounds in 30 days is ambitious, but entirely possible. It requires a steady, disciplined approach that combines a smart diet, targeted movement, and lifestyle tweaks. Here is your science-backed blueprint to hit your goal safely and keep the weight off for good.

Table of Contents
The Math Behind Losing 10 Pounds
To lose 10 pounds in a month, you must create a calorie deficit, meaning you burn more calories than you consume.
Generally, one pound of fat equates to roughly 3,500 calories. To lose 10 pounds in a month, you need to shed about 2.5 pounds per week, which requires a daily deficit of roughly 1,250 calories.
A Quick Reality Check: A 1,250-calorie deficit purely from food is too drastic and unsafe. The secret is splitting the difference: cut some calories from your diet and burn the rest through increased physical activity.
Refer to this Article from Science Focus for more scientific information.
1. Dial In Your Nutrition (Without Starving)
You can’t out-exercise a bad diet. To lose 10 pounds in a month, focus on high-volume, nutrient-dense foods that keep you full.
- Prioritize Lean Protein: Protein is your secret weapon. It boosts your metabolism through the thermic effect of food and keeps you satiated. Fill your plate with chicken breast, fish, tofu, eggs, and Greek yogurt.
- Load Up on Fiber: Vegetables, berries, legumes, and whole grains slow down digestion. This prevents blood sugar spikes and keeps random cravings at bay.
- Track Your Intake: Use a tracking app for just one week. You’ll be shocked at how quickly “healthy” handfuls of nuts, cooking oils, and liquid calories add up.
- Ditch Liquid Calories: Swap sodas, sugary coffees, and alcohol for water, black coffee, or herbal teas. This adjustment alone can easily cut 300 to 500 calories a day.
2. Optimize Your Workout Routine
To maximize fat loss while preserving lean muscle, you need a mix of strength training and cardio.
Lift Weights 3–4 Times a Week
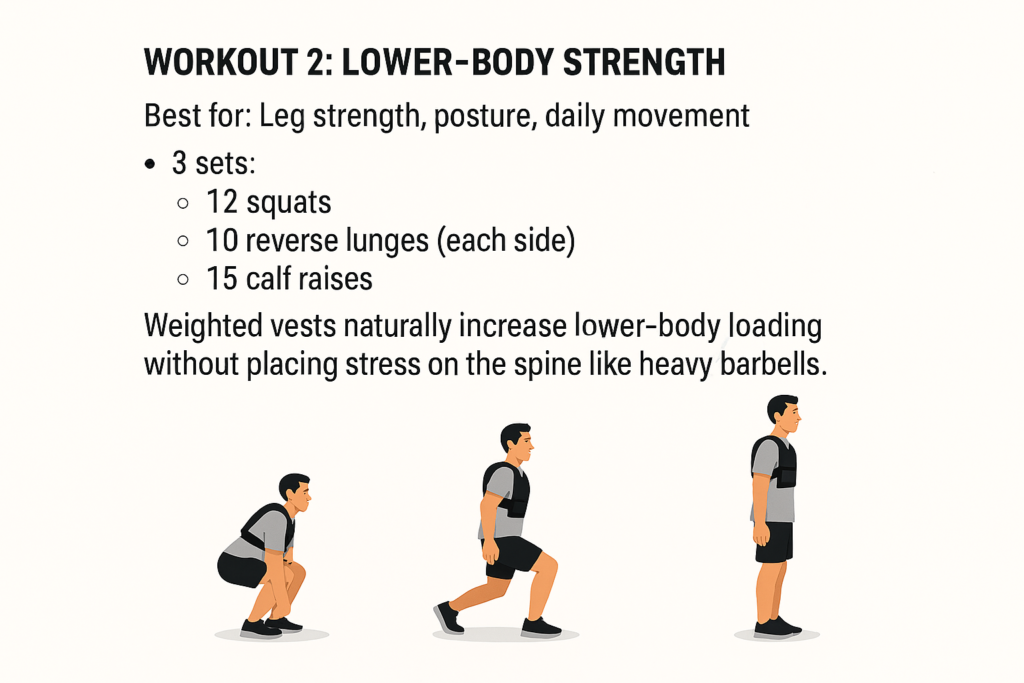
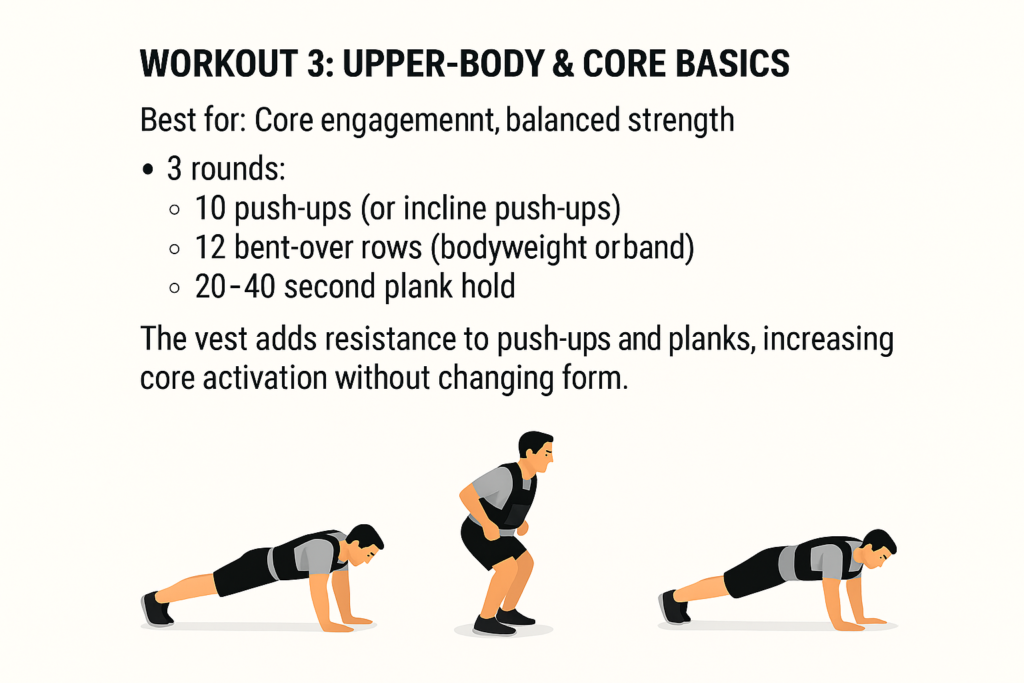
Muscle tissue burns more calories at rest than fat tissue. Focus on compound movements that recruit multiple muscle groups at once, such as:
- Squats and Lunges
- Push-ups or Bench Presses
- Rows and Lat Pulldowns
Increase Your NEAT (Non-Exercise Activity Thermogenesis)
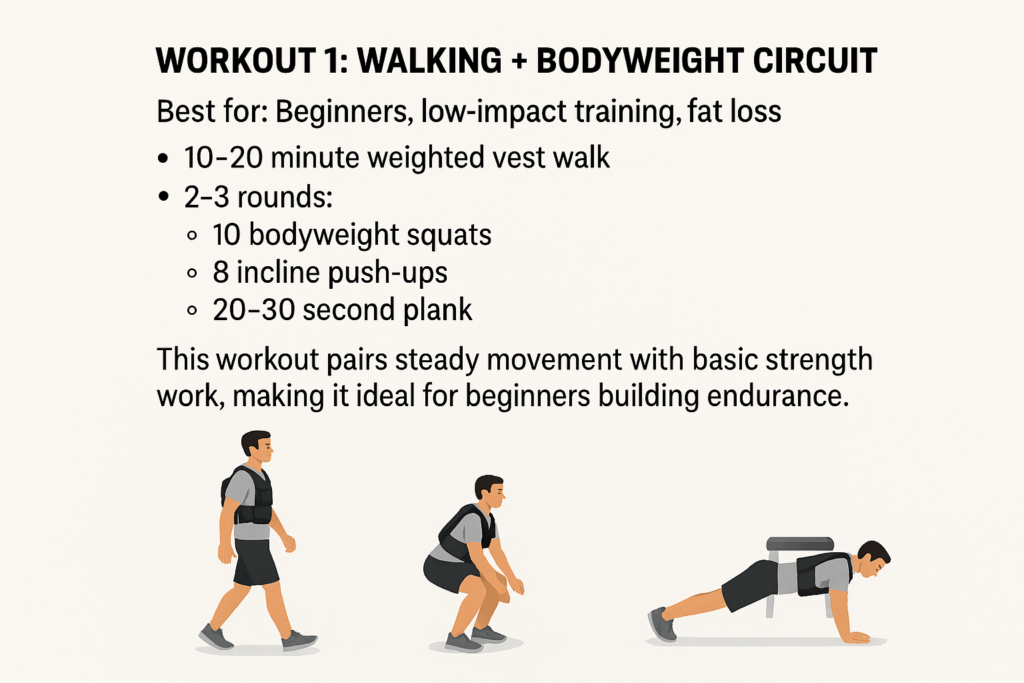
Structured workouts are great, but the movement you do outside the gym matters just as much. NEAT includes walking, cleaning, and pacing. Aim for 8,000 to 10,000 steps a day. Taking a 10-minute walk after each meal is an effortless way to hit this target.
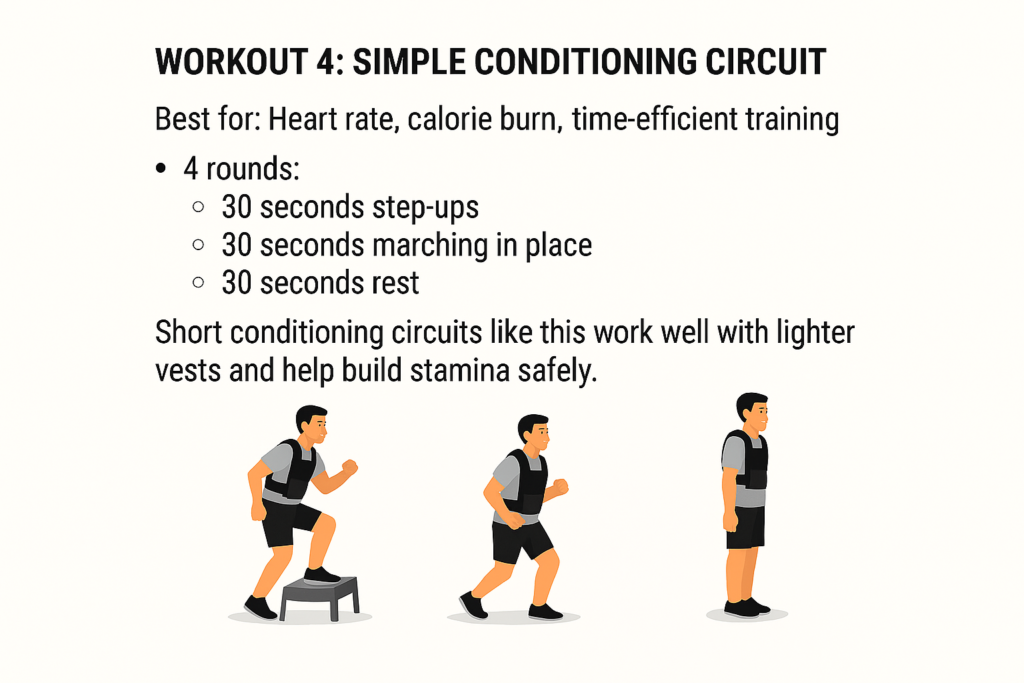
Add Strategic Cardio
You don’t need to run marathons. Add 20 to 30 minutes of moderate-intensity cardio (like brisk walking on an incline or cycling) after your weight sessions, or sprinkle in two short HIIT (High-Intensity Interval Training) sessions a week.
3. Master the “Invisible” Weight Loss Factors
If your diet and exercise are perfect but you aren’t losing weight, your lifestyle habits might be sabotaging you.
- Get 7–8 Hours of Sleep: Sleep deprivation spikes cortisol (the stress hormone) and ghrelin (the hunger hormone). When you are exhausted, your brain actively craves high-calorie, sugary foods.
- Manage Your Stress: Chronic stress triggers emotional eating and causes your body to hold onto visceral fat. Practice mindfulness, deep breathing, or simple outdoor walks to decompress.
- Hydrate Consistently: Mild dehydration is often mistaken for hunger. Drink a large glass of water 30 minutes before every meal to naturally control your portion sizes.
A Realistic 4-Week Timeline
Weight loss isn’t a straight line. Here is what you can realistically expect over the next 30 days:
| Week | What’s Happening to Your Body |
| Week 1 | The Initial Drop: You might lose 3–4 pounds quickly. This is mostly water weight and reduced bloating as you cut back on carbs and sodium. |
| Week 2 | The Adjustment Phase: Weight loss might slow down to 1–2 pounds. Your body is adapting to the calorie deficit. Stay consistent! |
| Week 3 | The Fat-Burning Zone: You’ll start noticing changes in how your clothes fit. Energy levels should stabilize as your metabolism adjusts. |
| Week 4 | The Home Stretch: By keeping your habits tight, you will approach or hit that 10-pound mark, feeling lighter, tighter, and more energized. |
Bottom Line: Consistency Wins
Can you lose 10 pounds in a month? Yes. But remember that the number on the scale is only one metric of success. If you lose 8 pounds of pure fat and build lean muscle, you will look and feel much better than if you starved yourself to lose 12 pounds of water and muscle.
Treat this month as the kickoff to a healthier, sustainable lifestyle. Focus on daily habits, celebrate the small wins, and let me-fitter.com guide you every step of the way.